Minimally Invasive Tests
A variety of tests are available to screen for possible pulmonary arterial hypertension associated with systemic sclerosis (PAH-SSc), to be followed by confirmatory right heart catheterization (RHC). They can be used at initial evaluation of SSc, regardless of PAH risk factors, and regularly to help identify the potential of associated PAH and trigger additional diagnostic tests before symptoms present.1-3
Pulmonary Function Tests (PFTs) FVC/Dlco ratio >1.6 and/or Dlco <60% of predicted may indicate a patient is at risk for PAH-SSc2
Echocardiogram with focus on the right heart may be used in patients with suspected PAH-SSc2
BNP or NT-proBNP Elevated biomarkers may indicate myocardial dysfunction2
PAH-SSc Screening Recommendations
Annual screening for PAH in patients with SSc is recommended:
The 2022 ESC/ERS Guidelines for pulmonary hypertension recommend patients with SSc have an annual evaluation for PAH (Class I recommendation)2
The Guidelines Also Provide the Following Recommendations2:
The Guidelines Also Provide the Following Recommendations2:
- In adult patients with SSc of >3 years' disease duration, an FVC ≥40%, and a Dlco <60%, the DETECT algorithm is recommended to identify asymptomatic patients with PAH (Class I, Level B recommendation)2*
- Assessing the risk of having PAH, based on an evaluation of breathlessness, in combination with echocardiogram or PFTs and BNP/NT-proBNP, should be considered in patients with SSc (Class IIa, Level B recommendation)2
- Policies to evaluate the risk of having PAH should be considered in hospitals managing patients with SSc (Class IIa, Level C recommendation)2
- In symptomatic patients with SSc, exercise echocardiography or CPET, or CMR may be considered to aid decisions to perform RHC (Class IIb, Level C recommendation)2
- In patients with CTD with overlap features of SSc, an annual evaluation of the risk of PAH may be considered (Class IIb, Level C recommendation)2
- In patients with SSc, where breathlessness remains unexplained following noninvasive assessment, RHC is recommended to exclude PAH (Class I, Level C recommendation)2
Confirming PAH-CTD Diagnosis
RHC is the gold standard test to diagnose PAH. It measures the blood pressure in the heart and pulmonary arteries, and is recommended in cases of suspected PAH-CTD to confirm diagnosis, determine severity, and rule out left-side heart disease.2,5
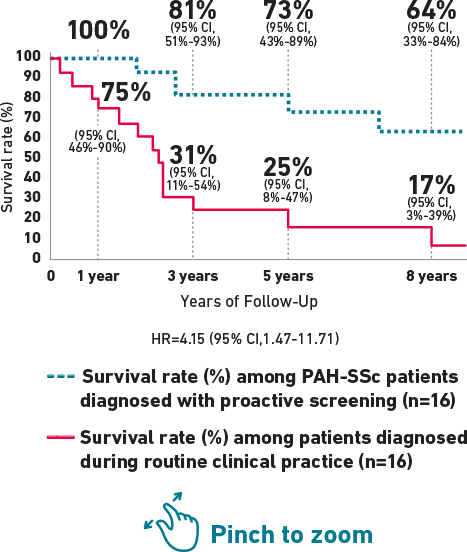
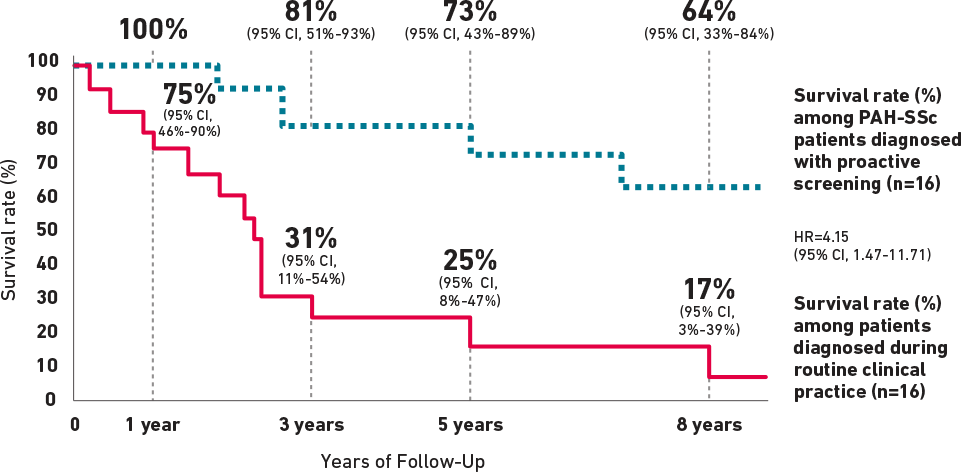
Survival Rates in Patients With PAH-SSc Diagnosed Through Proactive Screening vs Routine Clinical Practice
Retrospective analysis from the French PAH Registry and the ItinérAIR-Sclérodermie program showed higher survival rates in patients who were diagnosed with PAH-SSc with proactive screening in the detection cohort.6†
DETECT Video
Play the video below to understand the importance of regularly screening patients with SSc for PAH.